
Laparoscopic Ureterolithotomy – 2.5 cm Proximal Ureteral Stone
Laparoscopic ureterolithotomy for a large 2.5cm proximal ureteral stone. After mobilization of the colon, identification of the ureter and dissection of the inflammatory region when the stone is impacted. Opening of ureter using cold cut in order to obtain a neat incision and prevent thermal damage to the ureter.
Fascinating Laparoscopic Sacrocolpopexy (Grade 4 Bladder Prolapse)
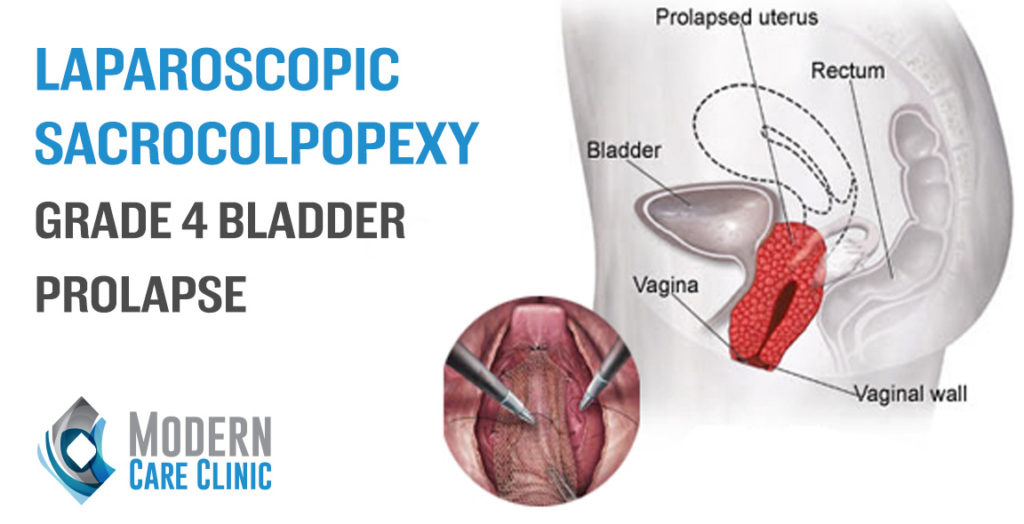
Laparoscopic Sacrocolpopexy, operated by Dr Fouad Khoury, in which he’s performing a laparoscopic pelvic organ prolapse repair. This video features anterior plane dissection for Grade 4 bladder prolapse using polyester mesh placement and fixation to sacral promontory.
Extraordinary Laparoscopic Pyeloplasty (Left)

Dr Fouad Khoury, a referral urologist in Lebanon and the Middle East, performing pyeloplasty for UPJ stenosis. This video features step by step approach along with captions for successful and smooth completion of pyeloplasty operation, with antegrade intra operative JJ insertion.
Superb Laparoscopic NephroUreterectomy (Left)

Laparoscopic NephroU done for management of upper tract TCC that was causing extensive bleeding and anemia for the patient. Due to advanced patient’s age (94 years old) and comorbidities, only a proximal ureterectomy was done after making sure that distal ureter is free of tumor in order to decrease operative time and surgical morbidity.
Amazing Laparoscopic Right Adrenalectomy (8 cm Tumor) Compressing Vena Cava

Laparoscopic right adrenalectomy of a large 8cm tumor compressing the Vena Cava. After dissection and isolation of adrenal gland from vital surrounding structures mainly the Vena Cava, hand assisted technique was used at the end in order to detach the adrenal from the posterior bed.
Impressive Laparoscopic surgery for adrenal gland – 7.5cm Tumor
Laparoscopic surgery for adrenal gland became the standard procedure for removal of adrenal tumors. When done in expert hands, even large tumors can be safely performed through this minimally invasive approach. It provides patients with less discomfort and equivalent oncologic results when compared to larger incisions required with traditional open surgeries.
Bladder prolapse expert | Dr Fouad Khoury
Dr Fouad Khoury discussing minimally invasive approach to repair pelvic organ prolapses such as cystocele and rectocele. The repair can be done either through a laparoscopic or robotic approach with a success rate higher than 90 percent when done in expert hands.
Urinary Incontinence

Urinary incontinence causes social distress. This is why many women do not discuss this problem with their doctor as they feel embarrassed.
Minimally Invasive Surgery

At Modern Care Clinic, we specialize in a wide range of services which cater to the fields of urology and minimally invasive surgery.
Robotic Surgery Congress in Lebanon Dr Fouad Khoury

Dr Fouad Khoury: President of the first robotic surgery congress in Lebanon and hosting Professor Alexandre Mottrie, CEO of ORSI academy, the largest robotic surgery training center in the world and President of the EAU Robotic Urology Section.