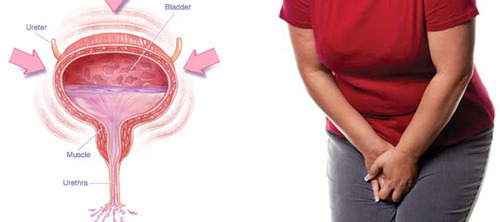
A cystocele or a prolapsed bladder occurs when ligaments that hold your bladder up and the muscle between a woman’s vagina and bladder are weak; for this reason, the bladder will fall into the vagina.
There are three grades of cystocele:
– Grade 1: The bladder falls only a short way into the vagina.
– Grade 2: The bladder falls to the opening of the vagina.
– Grade 3: The bladder comes out of the opening of the vagina; it’s a severe grade.
Causes and Risk factors
There are several causes and risk factors:
– Pregnancy and childbirth: Women who have had a vaginal delivery, multiple pregnancies, or whose infants had a high birth weight have a higher risk of anterior prolapse; because the pregnancy and the delivery may involve straining the muscles of the floor of the pelvis.
– Age: especially after menopause, when the production of estrogen decreases; so the muscles around the vagina are not strong anymore.
– Hysterectomy.
– Family history or genetic factor (some women are born with weak connective tissues).
– Obesity: Women who are obese are at higher risk of anterior prolapse.
– Constipation.
– Chronic coughing.
– Lifting heavy objects.
– Smoking.
What are the symptoms of a cystocele?
– Seeing something bloating through the vaginal opening.
Prolapsed Bladder can be diagnosed with a clinical history and a pelvic exam. The exam may be done while you are lying down, straining or pushing, or standing; the doctor may measure the severity of the prolapsed bladder by seeing in which part of the vagina the bladder has fallen.
Other tests and imaging studies may also be done to check the pelvic floor, and confirm the diagnosis of a prolapsed bladder:
– Cystoscopy: a long tube is passed through the urethra to examine the bladder.
– Urodynamics: to measure the capacity of the bladder to hold and release urine.
– X-rays
– Ultrasound
– MRI
How to treat the prolapsed bladder?
1- No treatment if the prolapse is:
– Not causing you problems.
– Not blocking your urine flow.
2- Behavior therapy
– Kegel exercises (which help the muscles of the pelvic floor to be strong).
– Pelvic floor physical therapy.
– Pessary: a vaginal support device to hold the bladder in place.
3- Estrogen replacement therapy
4- Weight loss
5- Surgery:
A moderate or severe prolapsed bladder may require reconstructive surgery to move the bladder into a normal position; and it can be performed through the vagina or the abdomen, under a spinal or general anesthetic.
The surgical treatment is the best therapy for bladder prolapse; but if a woman is planning for a pregnancy, surgery is contraindicated.
The patient usually goes home the day of the surgery, and the recovery time typically takes four to six weeks.
Diagnosis starts with a physical examination to evaluate your general state of health and identify any physical problems that may have consequences on your fertility. The doctor required the presence of the two partners and some tests:
Semen Analysis
Semen analysis is a routine lab test that helps to determine:
– Sperm volume, concentration, and count per ejaculation.
– PH of the sperm.
– Velocity: how fast your sperm travels.
– Morphology: Size and shape of your sperm.
– Color.
– Viscosity: liquefaction time of the sperm.
– Motility of the sperm.
– Viability of the sperm.
If the semen test shows low sperm numbers or the total absence of the sperm, it may not mean you are permanently infertile; more testing may be needed.
Transrectal Ultrasound
Your doctor may order a transrectal ultrasound. A probe is inserted in the rectum, and sound waves are delivered to the nearby ejaculatory ducts. This imaging technique can help the doctor to see if some structures such as the ejaculatory duct or seminal vesicles are blocked or present some problems.
Testicular Biopsy
If semen analysis shows oligospermia or azoospermia; you may need a testicular biopsy, which can be done with general or local anesthesia. A small cut is made in the scrotum, and a small piece of tissue from each testicle is removed and evaluated under a microscope. The biopsy helps to find the cause of male infertility; and to collect sperm for use in assisted reproduction (such as in vitro fertilization; IVF).
Hormonal Profile
The health care provider may check your hormones to know how well your testicles make sperm; by evaluating the FSH level (FSH is the pituitary hormone that tells the testicles to make sperm).
Can male infertility be treated?
When the diagnosis of male infertility is confirmed, the curative phase begins to increase the couple’s chance of having a child.
Depending on the cause of infertility, treatments may include:
Medications:
– Hormone therapy to increase the number of sperm, when infertility is caused by high or low levels of certain hormones.
– Treatments for sexual intercourse problems; when certain sexual problems in men cause infertility (premature ejaculation or erectile dysfunction), and in some cases the couple should consult a sexologist.
– Antibiotic treatments if there is an infection.
Surgical treatment :
For example, a varicocele can often be surgically corrected or an obstructed vas deferens repaired. Prior vasectomies can be reversed. When there is no sperm in the ejaculation, sperm can often be retrieved directly from the testicles or epididymis using sperm retrieval techniques.
– Assisted reproductive technology (ART): in ART sperm can be obtained through normal ejaculation, surgical extraction, or donor individuals, depending on your specific case and wishes. The sperm is then inserted into the female genital tract or used to perform in vitro fertilization or intracytoplasmic sperm injection (ICSI).
In IVF, the egg and sperm (of which there are many) fertilize on their own in the laboratory. In ICSI, the selected sperm is directly injected into the egg.
What about Fertility Preservation?
When you have medical and sexual issues that affect your fertility; freezing your sperm is the best method to preserve your fertility and increase the chance of having a child.
WHO IS A CANDIDATE FOR FERTILITY PRESERVATION?
Fertility preservation is an option when a man:
– Is diagnosed with cancer at a young age.
– Has sexual dysfunctions.
– Expects to have surgery especially a vasectomy.
– Has an autoimmune, hormone, or genetic disorder.
Nearly 1 in 7 couples is infertile, which means there is no pregnancy even though they’ve had frequent, unprotected sexual intercourse for a year or longer.
The male factor can be the cause of infertility, and this can lead to a stressful relationship.
When to see a doctor?
If no pregnancy after a year of regular unprotected intercourse, and if there is:
The most common problem is with the production and maturation of sperm. Sperm may:
– Not grow enough.
– Have a strange form.
– Not move the right way.
– We can have oligospermia (low number of sperm) or azoospermia (absence of sperm completely).
Sperm problems can be congenital; but sometimes a toxic lifestyle can reduce sperm count: smoking, drinking alcohol, and taking certain medications.
Other causes of low sperm numbers include long-term sickness (such as kidney failure), childhood infections, or hormonal testosterone disorder.
Damage to the reproductive system can cause low sperm numbers or the total absence of it ; which can cause the obstruction of the tubes that the sperm travel through.
Varicoceles
Varicoceles are overinflated veins located in the scrotum; they are more common in infertile men (40 out of 100). They stop the growth of sperm by blocking blood drainage and lead blood to flow back into your scrotum from your belly; the testicles are then too distended and hot to touch for making sperm, which can cause low sperm number.
Retrograde Ejaculation
Retrograde ejaculation is when semen goes into your bladder instead of out the penis. This happens when nerves and muscles in your bladder don’t close during orgasm; it can be caused by some procedures, medications, or health problems of the nervous system; signs are turbid urine after ejaculation and dry ejaculation.
Immunologic Infertility
Sometimes a man’s body makes antibodies that attack his own sperm because of a certain surgery or infection. Antibodies prevent sperm from moving and working normally in order to fertilize the egg.
Obstruction
Sometimes the tubes which sperm travel through can be blocked; some infections and surgeries (such as vasectomy) can cause blockage. Any part of the male reproductive tract can be blocked, which can lead to infertility because the sperm from the testicles can’t leave the body during ejaculation.
Hormones
A very low pituitary hormone level causes poor sperm growth.
Chromosomes defects
Hereditary disorders such as Klinefelter’s syndrome; in which a male is born with two X chromosomes and one Y chromosome (instead of one X and one Y) cause abnormal development of the male reproductive organs.
Medication
Certain medications have side effects on sperm production, function, and delivery. These medications help to treat:
– arthritis
– depression
– digestive problems
– infections
– high blood pressure
– cancer
Risk factors
Several factors can increase the risk of male infertility:
– Smoking.
– Abusing illegal drugs.
– Drinking alcohol.
– Don’t maintain a healthy weight.
– Being exposed to toxins.
– Overheating the testicles.
– Having a history of undescended testicles.
– Having genetic disorders.
– Having testicular injuries.
– Testicular cancer and treatment.
What are the complications of male infertility?
– Stress and relationship problems.
– Expensive and involved reproductive techniques.
– High risk of testicular and prostate cancer.
Prevention
Some measures must be taken into consideration to prevent infertility:
When you have these symptoms you should visit your urologist who will:
-Ask about your symptoms and your medical history.
-Do a physical exam for your abdomen, your rectum, and the organs in your pelvis.
-Bladder Diary: The patient should note how many times he goes to the bathroom and when he leaks urine; the bladder diary helps you track: when and how much fluid you drink, when and how much you urinate in 24 hours, how often you have the urgency feeling to urinate, when and how much you leak urine.
Other Tests
-Urine test: Your doctor will require a urine analysis and urine culture to determine if there’s a urine infection.
-Bladder scan: This ultrasound imaging shows how much urine is still in the bladder after you go to the bathroom.
-If there is any doubt about the diagnosis, the urologist required a cystoscopy or urodynamic testing.
Overactive Bladder treatment
Overactive bladder can interrupt your social life, but there are ways to combat the problem.
Natural Treatment for Overactive Bladder
-Bladder training: This type of training helps the patient to control the urge of urinating; he will able to control himself.
-Pelvic floor exercises: Called Kegels exercises; you tighten, hold, and then relax the muscles that you use to start and stop the flow of urination.
Drugs for Overactive Bladder
In the overactive bladder, we have contraction of the muscles in the bladder wall at the wrong time. A group of drugs called anticholinergics help by blocking the nerve signals related to bladder muscle contractions; these medications increase bladder capacity and decrease the urge to urinate.
To relieve dry mouth it is necessary to drink small amounts of water (because large amounts can worsen the symptoms of the overactive bladder) and suck a sugar-free candy; the doctor will recommend eye drops to relieve dry eyes and a diet rich in fiber for constipation.
Bladder injections
OnabotulinumtoxinA, also called Botox, is a protein injected in small doses directly into the bladder to relax the muscles. The effect of this protein lasts for 6 months so repeated injections are necessary.
Side effects of Botox injection: urinary tract infections and urinary retention.
Nerve stimulation
Helps to treat an overactive bladder by adjusting nerve messages from the brain to the bladder.
Surgery is required for people with severe symptoms who don’t respond to other treatments.
We have 2 types of surgeries:
-Surgery to increase bladder capacity by using pieces of your bowel to replace a portion of your bladder. This surgery is required only in cases of severe urge incontinence that doesn’t respond to any other treatment.
-Bladder removal: This procedure is the last solution of severe overactive bladder and consists of removing the bladder and surgically constructing a replacement bladder (neobladder) or an opening in the body to attach a bag on the skin to collect urine.
Some TIPS to prevent an overactive bladder
-Maintain a healthy weight.
-Do physical activities and exercises.
-Reduce your consumption of caffeine and alcohol.
-Stop smoking: smoking is irritating to the bladder muscle.
-Treat your chronic conditions, such as diabetes, that might lead to overactive bladder symptoms.
-Weak pelvic muscles: Pregnancy and childbirth can lead to the fragility of the pelvic muscles; so the bladder will sag out of its normal position. All of these factors can cause leakage.
-Nerve damage: Trauma and diseases (Parkinson’s, multiple sclerosis) can cause the damage of the nerves that sent signals to the brain and bladder to squeeze urine out of the body; so the patient will empty his bladder at the wrong time.
-Medicines that cause a rapid increase in urine production.
-Excess weight: The overweight causes extra pressure on your bladder. This can lead to urge incontinence.
-Hormonal deficiency in estrogen after menopause
Sometimes the doctor doesn’t find a cause for the overactive bladder.
Risk factors
-Age: You have a high risk of having an overactive bladder when you get older. Age also raises your risk of other conditions that affect bladder control: BPH, diabetes…
-Women have more risk of developing an overactive bladder than men for several causes that affect the hormones and the pelvic muscles: menstruation, pregnancy, and menopause.
-Obesity
-People who have certain diseases like stroke or multiple sclerosis.
Complications
Overactive bladder can affect your life and cause:
-Depression.
-Anxiety.
-Sleep disorders (Waking up often at night to pee).
First, the doctor will ask about the symptoms and the sexual activity of the patient; a urine analysis and urine culture will be required to prove the infection and determine the nature of the bacteria.
In case of recurrent UTIs, a doctor may request further diagnostic testing to determine the cause:
Diagnostic imaging: to assess the urinary tract by using ultrasound, CT and MRI scanning, radiation tracking, or X-rays.
Cystoscopy: This diagnostic exam helps the doctor to examine the lining of your bladder with a camera lens, which inserted through the urethra through a long thin tube.
Treatment of urinary tract infections in women
-Antibiotic: The patient will probably start taking the antibiotic before getting the results of his urine test.
When the results (accompanied by an antibiogram) are done, your doctor may change the prescription if the test shows that the bacteria causing your UTI is resistant to this antibiotic.
-Medications for pain relief.
-Drinking lots of water.
-Urinating frequently.
If the infection is not treated, it can lead to kidney damage.
In case of recurrent infections in women:
-Take a single dose of an antibiotic after sexual intercourse.
-Take a single, daily dose of an antibiotic for 6 months.
-Undergo estrogen therapy in case of menopause especially put vaginal eggs.
Some TIPS to reduce the risk of UTIs in women:
-Drink lots of water and urinate frequently.
-Reduce the quantity of alcohol and caffeine.
-Urinate directly after sexual intercourse.
-Wipe from front to back after urinating and defecating.
-Maintain good personal hygiene of the genital area.
-Sanitary pads or menstrual cups are preferred to tampons. Avoid using a diaphragm or spermicide for birth control.
-Not use any perfumed product in the genital area.
Robotic technology allows the surgeon to perform through the robot very precise and meticulous gestures with utmost accuracy; thus leading to excellent functional outcomes and very quick recovery as no painful incisions are made. Read More
Laparoscopic surgery
Laparoscopic surgery allows the surgeon to perform complex surgeries through small incisions. Recovery is very quick and with minimal pain as tiny incisions are being made. Very minimal scarring and quite esthetic. Read More
Prostate Laser surgery
Laser surgery for the prostate is a revolution that allows us to perform surgeries to the prostate while the patient is on blood thinners without the need to stop them, especially in patients who need to be continuously on such medications like Aspirin etc. Read More
Stone Laser surgery
Laser surgery for kidney stones eradicates the need to perform painful incisions in order to remove kidney stones and gives the advantage of being very accurate and incision free in most cases. Read More
Excess weight is associated with many comorbid conditions, such as heart disease, cholesterol imbalances, diabetes and the Metabolic Syndrome.. Read More
Diabetes Care
Worldwide, diabetes is on the rise, majorly due to an unhealthy lifestyle as well as predisposing factors. Read More






 Prostate Laser surgery
Prostate Laser surgery Stone Laser surgery
Stone Laser surgery Sexual Health
Sexual Health